It can be diagnosed by the following tests, and these tests are aimed to find the cause of the cancer in a molecular level.
1. Physical exam and history of the patients' habits, previous illnesses and treatments.
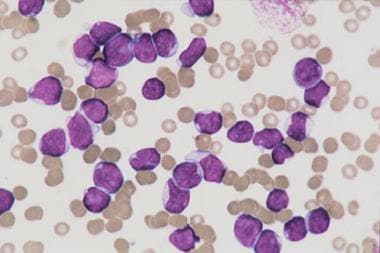
2. Complete Blood Count: A test that measure the number of red blood cells, platelets, the amount of hemoglobin, and the number and types of white blood cells.
3. Cytogenetic analysis which view sample of blood and or bone marrow under microscope in laboratory to chick any genetical mutations.
4. Bone marrow aspiration and biopsy.
5. Immunophenotyping.
6. Blood chemistry studies.
Metastasis happens when cancer cells spread outside of the blood, and there are three ways cancer cells spread in the body:
1. Cancer cells invade solid tissues such as brain and heart through the blood vessel.
2. Cancer cells can also invade lymph system by spreading in the lymph vessel and form solid tumor.
3. Cancer cells that have invaded solid tissues and formed tumor can also invade neighboring tissues and organs.
2.3: What are the risk groups that classify the treatments of patients with Pediatric Acute Lymphoblastic Leukemia? (1) (2)
There are two risk groups that are used to design treatment plans for children with pediatric acute lymphoblastic leukemia.
1. Low risk group:
- Children from 1- 9 years.
- White blood cells count < 50,000/µL at diagnosis
2. High risk group:
- Children < 1 year
- White blood cells count equals or are more than 50,000/µL at diagnosis.
There are four different standard treatments:
1. Chemotherapy.
2. Radiation therapy.
3. Chemotherapy with stem cell transplant.
4. Targeted therapy. (Using drugs or substances that target cancer cells only)
2.5: What are the new types of treatment for Pediatric Acute Lymphoblastic Leukemia? Are they being used? (2)
These new treatments that are in clinical trials are High-dose chemotherapy and Targeted therapy. Patients may choose to be part of these clinical trials, and follow-up tests are needed to check the rate of the recovery and how far these treatments can go.
2.6: What is a Recurrent or Relapse Pediatric Acute Lymphoblastic Leukemia and what is the treatment for it? (1) (2)
Recurrent or Relapse Pediatric Acute Lymphoblastic Leukemia is when the cancer recurred after treatments. When cancer returns, it can be spread to blood, bone marrow, testicles, brain and spinal cord.
These are the standard treatments:
1. Chemotherapy and radiation therapy. (When cancer spreads in testicles only)
2. Chemotherapy and intrathecal chemotherapy with radiation therapy. (When cancer spreads in brain and or spinal cord only)
Work Cited:
(1) Childhood Acute Lymphoblastic Leukemia Treatment (National Cancer Institute) http://www.cancer.gov/types/leukemia/patient/child-all-treatment-pdq
(2) Childhood Acute Lymphoblastic Leukemia: Learn the Symptoms (MedicineNet) http://www.medicinenet.com/childhood_acute_lymphoblastic_leukemia/article.htm



{kind=link}
{kind=link}