What made me interested in writing this blog is that I visited children with leukemia at a hospital in the capital city of my country. I saw how these children were keeping up with their treatments, and how their family were always worried about the treatments' result. I wanted to learn more about the available treatment courses, especially that they are related to my major. By writing each chapter in this blog, I can say that I have developed a background on this topic, and that I can confidently answer anyone who has questions about pediatric acute lymphoblastic leukemia. I truly have learned many things about this topic. How does this cancer work? Why it is named by this? What are the available treatments? Are there any limitations to the available treatments? What are the costs of the available treatments? And so on. I genuinely hope that whoever stops by and reads my blog gets a decent idea of pediatric acute lymphoblastic leukemia. I also would like to thank everyone who has read and spent his and her time commenting on my blog. Image Source:https://blogger.googleusercontent.com/img/b/R29vZ2xl/AVvXsEg5nVzqWu_bBo89DQnNDVkDVNzma1AA8A3X0rs_Qr9lqCzJhVsCtiouOsPBaPuZgI_xtp3jmfb3CDr6J-ZaX98gG8iVDm-1pFNWLon1pwvp0AzYn2XxvF3f7gegew5wRXpHTZFnxLSYltV4/s1600/618_final_thought.jpg
In the article "Genetics May Help Guide Kid's Cancer Treatment" on the U.S. News, the author finds that researchers and doctors claim that genetics may help guide and instruct the treatment course of children with cancer. It is stated in the article that a study on genetic sequencing has revealed potential findings on half of the children with aggressive cancer. These potential findings are critical because they are the answers to why their treatments are not working on them, and some of them may go through a new diagnosis because genetic mutations that cause their cancer to progress have been detected. As a result, 10% of these children have undergone new treatment, targeted therapy, and are introduced with new drugs. Some of them have temporarily fought the cancer and some of them have had a complete remission. Treatments that are based on genetics findings are personalized because each patient has mutations that are different from another patient that have the same cancer. Researchers and scientists will do their best to find new treatments that hopefully may 100% cure cancers. Targeted cancer therapy and immunotherapy are examples of the newly developed treatments. In the article, it mentions that cancer cure rate has increased overtime. In 1960s, the cure rate of pediatric acute lymphoblastic leukemia was less than 10%. Today, the cure rate has increased to 90%. The article covered concerns that parents may have. The time, the result and the cost of undergoing these clinical trials are always the patient's family's main concerns. The author mentions that in the study, 91 pediatric cancer patients in Mott Children's Hospital are undergoing newly designed treatments. The study reports that around 46% of the children who have taken genetic tests have available treatments that target their mutations. However, the study hasn't reported the reasons why the rest couldn't receive treatments. Is it because targeted drugs are hard to develop or is it because the children's bodies are resistant to the drugs? The study mentions the cost of this clinical trail, and it is around $6,000 and it takes 50 days for each patient. The result of this study is, some of the children have partial remission and some have complete remission. The author also brings up an important point. Can children undergo targeted cancer therapy? Are these drugs, big pills, suitable for children? Is it safe for younger children to undergo these clinical trails? The study that is mentioned in this article unfortunately hasn't mentioned any of these concerns. Article Source: http://health.usnews.com/health-news/articles/2015/09/01/genetics-may-help-guide-kids-cancer-treatment Images Source: (1) http://32f7sg2by83y1dtg9mdxf11m.wpengine.netdna-cdn.com/wp-content/uploads/2012/06/Genetics.jpg (2) https://d3f1iyfxxz8i1e.cloudfront.net/courses/course_image/7d90511e6193.jpg
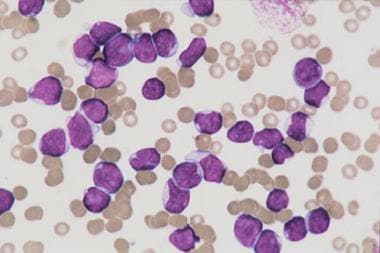
Q: What does leukemia mean? A: Leukemia is a blood cancer. More specifically, it is a cancer of the bone marrow in which the blood cells are grown and developed. Some of these blood cells, white blood cells, grow in a very rapid speed and become immature cells that then disrupt the functions of mature blood cells. Q: What causes Pediatric Acute Lymphoblastic Leukemia? A: The causes of leukemia are still unknown. However, there are possible factors that lead to leukemia which are the genetic mutation in patients' chromosome, pregnant mothers' exposure to radiations, past treatment with chemotherapy, and having genetic mutation such as Down syndrome could be a possible cause of leukemia. Q: What are the available treatments for Pediatric Acute Lymphoblastic Leukemia? A: There are four standard treatments for Pediatric Acute Lymphoblastic Leukemia which are chemotherapy, radiation therapy, chemotherapy with stem cell transplant, and targeted cancer therapy. Q: What is targeted cancer therapy? A: Targeted cancer therapy is a therapy in which drugs or other substances are used to interfere with molecular targets that cause the growth of cancer cells by blocking them. Q: What are the limitations to targeted cancer therapy? A: Targeted cancer therapy is still in clinical trails and it has limitations. One of which is that molecular target's structure can be resistant to the drugs. Secondly, mutation in the molecular target could occur. When mutation happens, cancer cells find new and different pathway to grow even more rapid than before. Lastly, some molecular targets are complexed structure, thus developing a drug is hard and complicated. Q: What is immunotherapy? A:Immunotherapy is a newly developed therapy in which drugs or components are introduced to patients' body to stimulate some parts of their immune system to fight back cancer. Q: What does it mean that the treatment is in a clinical trial? A:When treatment is in a clinical trail, it means that researchers are still developing the drugs and clinical outcome is yet unknown. Researchers are also still studying the causes of the disease and try to link and evaluate these causes with the safety of the developed drugs they provide. References: (1) Childhood Acute Lymphoblastic Leukemia Treatment (National Cancer Institute) http://www.cancer.gov/types/leukemia/patient/child-all-treatment-pdq (2) Childhood Acute Lymphoblastic Leukemia: Learn the Symptoms (MedicineNet) http://www.medicinenet.com/childhood_acute_lymphoblastic_leukemia/article.htm (3) Clinical Trials: What You Need to Know (What You Need to Know about Clinical Trials)
In the article "T-Cell Immunotherapy Cure for Cancer" on MIT Technology Review, it is discovered that T cell immunotherapy has a successful cure rate on a patient who has reemission of acute lymphoblastic leukemia. Immunotherapy is an approach to use gene therapy to make immune system targets cancer cells in patients’ body. The study then conducts on around 61 patients with leukemia or lymphoma. Hans Bishop, a former Bayer executive who is the Juno company’s CEO states that the reassigns of this therapy’s success are unknown. Additionally, Bishop asserts that the study has small participants, and it doesn’t have a control group to conduct a comparison. The study, however, shows positive outcomes. Bishop claims that this new approach has opened new paths for treating and curing cancers. This approach uses living cells as drugs to attack cancerous cells. In this case, researchers use engineered T cells to fight back leukemia. T cells are part of the immune system cells.
Juno is not the only company that conducts clinical trails on this approach. There other 30 companies use immunotherapy to fight back other types of cancerous cells. In the article, it indicates that the cost of preparing a dose of T cell ranges from $50,000 to $75,000. Juno announces that researchers will conduct 10 studies on six types of T cells, and test it not only on patients with leukemia, but also on patients with different types of cancer. The company's new aim is whether or not this type of treatment works on other types of cancer as well. Novartis and Penn report that low doses of engineered T cells haven't shown any effects in five patients with cancers of the pancreas, ovaries, or lung. However, this study is still in its initial clinical trials.
At Dendreon corporation, the modestly effective treatment costs around $90,000. The article states that the manufacture costs half of that price, and company declares its bankruptcy last year. They had 400 staff members to work in developing gene and cell therapy. On the other hand, Citygroup analyst estimates the cost of dose of genetically engineered cells is around $500,000. Comparing to chemotherapy's hospital bills that could cost up to $2 million, immunotherapy is cheaper. Chemotherapy recovery lasts for a year or so and could cause complications to patients' organs, whereas immunotherapy is cheaper, has positive effects and doesn't cause organs damages.
Article Source:
A T-Cell Immunotherapy Cure for Cancer | MIT Technology Review (MIT Technology Review)
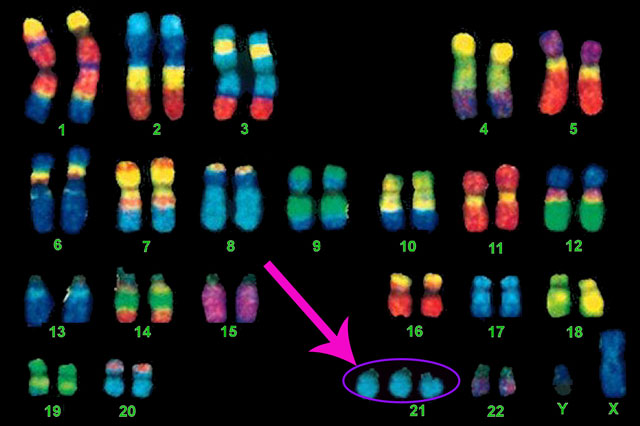
As mentioned in the previous chapters, one of the possible factors that leads to pediatric acute lymphoblastic leukemia is when a child has a genetic condition or disorder such as Down Syndrome. Down syndrome or more specifically a genetic disorder and abnormality in the number of chromosome 21. Instead of having two copies of chromosome 21, children with Down syndrome have three copies of it. Therefore, this genetic disorder is also referred to a constitutional trisomy 21 in medical journals.
After a case reported and published in 1930 to relate the susceptibility of having leukemia when the patients have a genetic condition such as Down Syndrome, the link between leukemia and genetic disorder has been questioned and become a spotlight when conducting a research.
Researchers compared two groups of leukemia patients. They compared toxicity level and side effects of chemotherapy between Down syndrome leukemia patients and non-Down syndrome leukemia patients. The result is children with Down syndrome who have leukemia have high and increased level of toxicity to chemotherapy drugs compared to patients who don't have any type of genetical disorders.
Children with Down syndrome lack genes that are important for expressing other significant genes or hormones in their bodies. One of which is GATA1. These children have mutations in this gene. Researchers have compared children with leukemia who lack this gene and children with leukemia who do not have genetical disorder. Children who lack this gene couldn't express other genes that help them to recover from chemotherapy drugs. The level of gene expression is very low compared to the control group. The link between mutations in the gene GATA1 and treatment-related toxicity is not understood at first.
Now that the relationship between lacking the gene GATA1 and experiencing toxicities to chemotherapy is being understood, researchers are trying to develop new chemotherapy drugs that decrease the treatment-related toxicities and prevent relapse pediatric acute lymphoblastic leukemia patients with Down syndrome.
Article Source:
(1)Acute leukemia in children with Down syndrome (Haematologica)
One of the possible factors that lead to Pediatric Acute Lymphoblastic Leukemia is when a child or a patient has a chromosomal defect or any types of genetic mutation in his or her chromosomes. Interestingly, I found an article on ScienceDaily that has published last month on 24th of September claims that researchers have found how defect or mutation in a certain chromosome leads to blood cancer. This finding could change the future treatments’ journey and development. Many of the leukemia cancer patients have partial deletion on their chromosome 9 in this study case. Their body can not express and produce the tumor suppressor hnRNP K that controls the spread of cancerous cells. "Our findings showed that hnRNP K haploinsufficiency led to tumor development by deregulating cell proliferation and differentiation programs through control of key cellular pathways,…" assert and claim by the researchers at University of Texas M. D. Anderson Cancer Center. Now, what's next? Can this tumor suppressor be developed in laboratories? How safe is this treatment? These are the questions that ring in my head after reading the article. This treatment falls under targeted cancer therapy because it is a drug that is introduced to patient's body to stop the cancer cells from rapidly growing and spreading to other tissues. However, targeted cancer therapy has some limitations. Some patients develop resistance to some drugs. Another limitation is that some molecular targets develop mutation and find new pathway to develop and spread more cancer cells. Lastly, sometimes it is hard to develop a drug that targets complicated molecular targets due to their structural complexity. Is the protein coding- gene hnRNP K a complex molecule? The article hasn't stated yet any thing about these concerns. Patients' family and guardians may be concerned about the effectiveness and the success rate of this drug. However, since this discovery is recent, patients will have to wait for the upcoming hopeful news. This news could change their fate and treatment courses.
2.1: How is Pediatric Acute Lymphoblastic Leukemia diagnosed? (1)(2)
It can be diagnosed by the following tests, and these tests are aimed to find the cause of the cancer in a molecular level.
1. Physical exam and history of the patients' habits, previous illnesses and treatments.
2. Complete Blood Count: A test that measure the number of red blood cells, platelets, the amount of hemoglobin, and the number and types of white blood cells.
3. Cytogenetic analysis which view sample of blood and or bone marrow under microscope in laboratory to chick any genetical mutations.
Metastasis happens when cancer cells spread outside of the blood, and there are three ways cancer cells spread in the body:
1. Cancer cells invade solid tissues such as brain and heart through the blood vessel.
2. Cancer cells can also invade lymph system by spreading in the lymph vessel and form solid tumor.
3. Cancer cells that have invaded solid tissues and formed tumor can also invade neighboring tissues and organs.
2.3: What are the risk groups that classify the treatments of patients with Pediatric Acute Lymphoblastic Leukemia? (1)(2)
There are two risk groups that are used to design treatment plans for children with pediatric acute lymphoblastic leukemia.
1. Low risk group:
- Children from 1- 9 years.
- White blood cells count < 50,000/µL at diagnosis
2. High risk group:
- Children < 1 year
- White blood cells count equals or are more than 50,000/µL at diagnosis.
2.4: What are the different types of treatment for Pediatric Acute Lymphoblastic Leukemia? (2)
There are four different standard treatments:
1. Chemotherapy.
2. Radiation therapy.
3. Chemotherapy with stem cell transplant.
4. Targeted therapy. (Using drugs or substances that target cancer cells only)
2.5: What are the new types of treatment for Pediatric Acute Lymphoblastic Leukemia? Are they being used?(2)
These new treatments that are in clinical trials are High-dose chemotherapy and Targeted therapy. Patients may choose to be part of these clinical trials, and follow-up tests are needed to check the rate of the recovery and how far these treatments can go.
2.6: What is a Recurrent or Relapse Pediatric Acute Lymphoblastic Leukemia and what is the treatment for it? (1)(2)
Recurrent or Relapse Pediatric Acute Lymphoblastic Leukemia is when the cancer recurred after treatments. When cancer returns, it can be spread to blood, bone marrow, testicles, brain and spinal cord.
These are the standard treatments:
1. Chemotherapy and radiation therapy. (When cancer spreads in testicles only)
2. Chemotherapy and intrathecal chemotherapy with radiation therapy. (When cancer spreads in brain and or spinal cord only)
In the bone marrow, blood stem cells are formed. These cells are immature cells and overtime, they develop and become mature blood cells. They may become either myeloid stem cells or a lymphoid stem cells.
When myeloid stem cells develop, they become one of these cells: Red blood cells (carrying oxygen), Platelets (blood clotting), or Granulocytes (fighting infection and disease). On the other hand, when lymphoid stem cells are developed, they become T lymphocytes (help B lymphocytes), B lymphocytes (produce antibodies) and Natural killer cells (kills foreign bodies).
1.3: What is happening in a children’s bone marrow with Pediatric Acute Lymphoblastic Leukemia? (1)
In children’s bone marrow with acute lymphoblastic leukemia, more of their blood stem cells develop into immature lymphoblasts, B lymphocytes, or T lymphocytes. As a consequence of having many of these leukemia cells, white blood cells, red blood cells, and platelets do not have space to flow in the blood stream. Cancer cells or leukemia cells do not fight infection or disease as the normal lymphocytes cells do. As a result, blood infection, anemia and bleeding occur.
1.4: What are the factors that lead to Pediatric Acute Lymphoblastic Leukemia? (1)
These are possible factors that cause pediatric acute lymphoblastic leukemia such as being exposed to x-rays or radiation before birth, genetic mutation in the chromosome. Also having genetic condition such as down syndrome, bloom syndrome, shwachman syndrome, Ataxia-telangiectasia or Neurofibromatosis type 1 (NF1) may lead to pediatric acute lymphoblastic leukemia. Another possible factor could be from a result of past treatment with chemotherapy. (1)
1.5: What are the signs and symptoms of a child with pediatric acute lymphoblastic leukemia? (2)(3)
These are the possible signs and symptoms that appear to a child with pediatric acute lymphoblastic leukemia which are fever, bruising and bleeding easily, dark spot under the skin, loss of appetite and weakness. The child looks pale and is always tired. The child also suffers from bone or joint pain. Lumps appear in the neck, underarm, groin or stomach of the child. These lumps are not painful.(2)
1.6: What are the factors that affect of the chance of the recovery and the treatment? (1)
The prognosis depends on several factors such as age, gender, race, the number count of the white blood cells in the blood, the type of lymphocytes where the leukemia cells begin to grow from. Mutation in the chromosomes or the genes of the lymphocytes has a great affect on the prognosis. The rapid growth of the leukemia cells should decrease after the initial treatment also affects the rate of the recovery. (1)
The treatment options also depend on the factors that affect the prognosis. The age of the child at the diagnosis plays a role on the treatment options. The decrease in the leukemia cells count after the initial treatment and the type of lymphocytes that the leukemia cells begins to divide and grow affect how the treatment options will be designed.(1)
After reading this chapter, to test your general knowledge about Pediatric Acute Lymphoblastic Leukemia, click on "QUIZ" or use the URL.


{kind=link}









{kind=link}
{kind=link}